Content
Traditional vs flipped
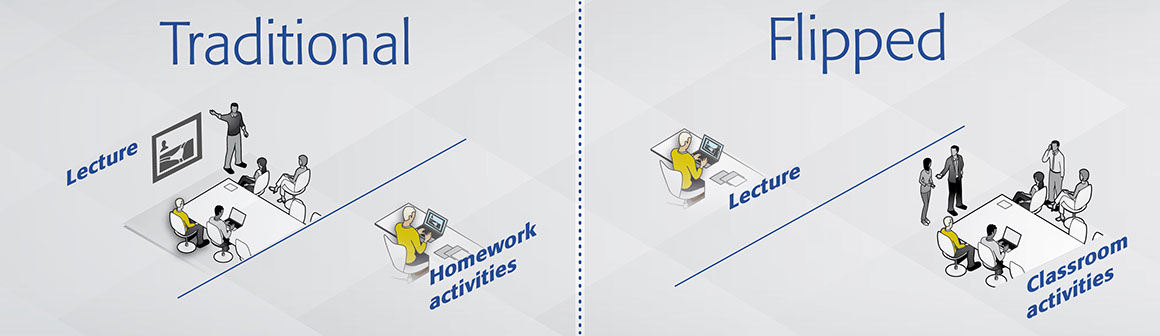
Traditional
• Faculty instructs
• Learners take notes
• Learners follow guided instructions
• Faculty gives assessment
• Learners have homework
Flipped
• Faculty instructs lesson at home (video/podcast/book/website)
• Learners work in class
• Deeper understanding of concepts, applications, and connections to content are made.
• Students receive support as needed
Traditional and flipped teaching models: in a flipped classroom, class-time and self-study activities are reversed or "flipped". (Adapted from: University of Washington, USA)
Turning learning upside down: the flipped classroom and what it can offer medical education
Read an interview with
Charles Prober …
Read the counterview by Brian McGowan …
The proliferation and diversification of technologies is changing the way people teach and learn the world over. Internet and computer accessibility has created a myriad of educational opportunities that were not available even a few short years ago. Technology is changing how students learn, as well as how educators teach, and this evolution has made new educational models such as the flipped classroom possible. A flipped classroom is where lectures are viewed outside of class and the application of material takes place during class sessions; a reverse or flip of traditional educational models.
In practice activities in a flipped classroom can take many forms, but generally involve learners preparing for courses by watching a prerecorded lecture or undertaking assigned reading and eLearning activities, followed by class time being used for interactive discussion, problem-solving, and other activities with the faculty. The flipped classroom puts more responsibility of learning on the learner and allows the teacher/educator more time to work one-on-one with learners.
Developed in the US
Two high school chemistry teachers from Colorado first popularized the flipped classroom model in 2007. Aaron Sams and Jonathan Bergmann were initially seeking a solution for students who had to miss class due to sports or other activities. When they began using screen capture software to record their lectures and Power Point presentations and post them online they realized that they could then use valuable class time to focus more on the application of the content learned in the video lectures. Flipping the classroom also allowed Sams and Bergmann to track individual students more closely and create more individualized lessons or problem sets for students.
The first large-scale test of the flipped classroom model came just three years after Sams and Bergmann first flipped their chemistry classes. Clintondale High School in Michigan was struggling with high failure rates for students in all disciplines for years before they decided to test the flipped classroom model. They began in 2010 by flipping courses for incoming freshman students.
Decreased failure rates
This proved so successful that they decided to flip the entire school starting the next year and the results were dramatic. In one year, the student failure rate in English went from 52% to 19%, in math from 44% to 13%, in science from 41% to 19%, and in social studies from 28% to 9%. Clintondale was able to decrease the average student failure rate by over 25% with very little extra resources and almost no additional expenditures.
Benefits for all parties
Advantages of the flipped classroom approach are centered around the change of time used during class sessions and include:
• An increase in interaction between learners and teachers
• A shift in the responsibility for learning on to participants
• The ability for learners to prepare at a time that suits them, and as many times as meets their needs
• Lessons and content are most accessible and archived
• Promotes student-centered learning and collaboration between students
• An increase in learner engagement and a shift from passive listening to active learning
Wide-range of online resources
The explosion of YouTube and development of online video educational resources, such as Khan Academy, have greatly facilitated the expansion of the flipped classroom model. Instead of having to prerecord all their lectures, teachers and instructors are able to choose from a variety of video lectures on a wide range of subjects to use for their courses. Enabling the teacher to act as a curator of lecture material (as opposed to the primary author) aids in the transition from the "sage on the stage" to the "guide at the side."
Used by post-secondary institutions
The flipped classroom model is now gaining popularity in higher education. A number of universities offer courses using the flipped classroom model and are examining the approach for various disciplines. At the University of British Columbia in Canada, two sections of a large enrollment introductory physics class were compared. One section used the flipped classroom model for one week, while the control section maintained traditional lecture-based format.
The researchers found that students in the flipped classroom section performed better on an end of week test (scores of a mean of 74% versus 41% for the control section), had higher rates of attendance (75% vs 53%), and higher levels of engagement (85% vs 45%).
Positive student feedback
Utilization of the flipped classroom model in an integrated pharmaceutical care and science course showed that students both performed better on tests and had more positive perceptions about the model compared to students taught in previous years using a traditional lecture-based teaching model.
Pharmacology students performed significantly better on the final exam (average score of 81,6% vs 77,7%) when taught using the flipped classroom model. Students who experienced the flipped classroom model generally liked it and over half of the students expressed a desire to have more instructors flip their courses.
Some criticism
Critics of the flipped classroom model assert that simply rearranging what part of learning is done where does not necessarily change learning outcomes. The potential need to invest time to develop courses (or redesign course format) and resources for technological investment are two frequently cited reasons why teachers are hesitant to adopt the flipped classroom model. Key to the success of this approach is that participants take responsibility for their learning and come to class prepared.
References
[1] Deslauriers L, Schelew E, Wiesman C (2011) Improved Learning in a Large-Enrollment Physics Class. Science. 13;332(6031):862–4.
[2] Pierce R, Fox J (2012) Vodcasts and Active-Learning Exercises in a “Flipped Classroom” Model of a Renal Pharmacotherapy Module. Am J Pharm Edu V 76(10) Article 196.
A "buzzword" for several years, the flipped classroom is currently being tested in a variety of educational settings.
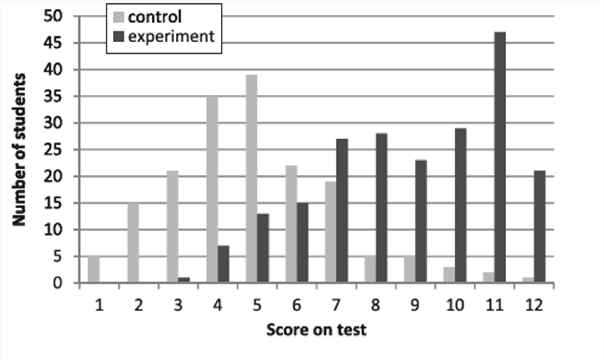
Flipped classroom improves learning
Test scores (out of 12 questions) for students in a lecture-based (control) and flipped (experiment) large-enrollment physics course. The highest scores were obtained from those who learned the content via the flipped classroom model.


The flipped classroom in medical education
"People must have sufficient education to participate in rich discussion."
One of the most vocal proponents for using the flipped classroom model in medical education is Dr Charles Prober, senior associate dean at Stanford School of Medicine. Prober argues that while medicine and the amount of information that students are expected to learn and understand has multiplied many times over, the way that medical education is conducted has not changed significantly in the last 100 years.
AO: What led you to rethink the way medical school is taught?
Dr Charles Prober : The main impetus was the need to deliver content in a way that is more tailored to the individual learner and then to bring learners together in a more compelling environment. People must have sufficient education to participate in relevant discussion. I believe that people can acquire foundational information in an asynchronous way; whether it’s by reading a text book, watching short videos, or other strategies that play to their particular learning. The more important part is to bring the learners together in some richly interactive forum to take care of patients—either having part of their education be taking care of patients or the simulation of the taking care of patients.
What are the greatest advantages of a flipped classroom model for medical education?
One advantage is that you can scale the delivery of the core knowledge. A library of short videos can be delivered to any number of people through online platforms. Not only can you scale up to more learners, but you can transport it to every region of the world that this is relevant to. The important part of the interactive piece is that it plays to the local population of learners whether it’s in a particular medical center or particular part of the world. They can interact with the material in situations that are relevant to their learning level and the learning environment.
How has Stanford School of Medicine used the flipped classroom concept?
We’ve used it in a number of different environments so far: for medical students, residents and fellows, and even beginning in continuing medical education. Our medical student biochemistry course has been converted from in-class lectures to a set of short videos that then are complemented by in-class sessions where the class solves problems using their biochemistry knowledge in the context of patients with metabolic diseases to make it clear that biochemistry does indeed have relevance to the practice of medicine. For several years that course was poorly rated by the majority of students; 80% of felt that the course was not particularly good and did not attend. Last year the net proportion of students who were very satisfied was in excess of 80%! Attendance was not mandatory for the interactive sessions with problems given in the context of real patient issues, yet about 95% of students did attend. It really is a reversal of fortune for that particular class.
What lies ahead for the flipped classroom concept at Stanford?
Our next big project, which we just launched, is actually a multi-medical school collaborative bringing together five schools to work through a big chunk of the preclinical curriculum in microbiology and immunology. Then we are going to transfer the material which is factual or foundational into a library series of short videos. We will develop in-classroom exercises and then we will implement the curriculum in the five schools and measure the outcome. We hope to implement this curriculum in the next academic year.
How can continuing medical education benefit from the flipped classroom model?
The online part of a course provides the opportunity to reach many more people than would come to more standard CME offerings. I think much of what we deliver in CME is factual based information; one could deliver that factual information before a course and then use the meeting time to really work through it and problem solve. The opportunity is to take it to the next level and we are just beginning that journey.
Charles Prober MD
Charles G Prober, MD is senior associate dean, medical education and a professor at Stanford School of Medicine. He is interested in medical education at all levels (undergraduate, graduate, residency, and fellowship). His clinical education focus centers on microbiology and pediatric infectious diseases and on the education of clinical research scientists.
"Flipped classrooms are not a miracle cure."
Why the flipped classroom model for medical education?
McGowan: While there has been tremendous progress made in the way medical education content is developed and delivered, thereare still significant barriers in place that prevent it from having the impact needed. To be frank: way too much is expected of learners and way too little is expected of teachers. From that perspective,educational models that better structure new content and the learning experience for the student will go a long way to simplifying knowledge transfer,
What are the biggest challenges of using a flipped classroom in medical education?
By its simplest definition, the flipped classroom IS NOT all that innovative. If all you do is put lectures online and then produce inflexible live “interactive” learning session then you WILL fail. The secret is not in the order of the learning experiences; the secret is in what that order allows you to do as an educator. Flipping the classroom allows you to leverage learning analytics (from the upfront and online content) to reshape or even individualize the live, face-to-face learning environment. Add to this the reality that facilitating a live, interactive learning lab is not something that every Faculty member is comfortable doing, and you have a lot of ways that this can all go horribly wrong. Flipped classrooms are not a miracle cure…the ‘angel’ is in the details.
Are there other tools you think are beneficial for medical education?
For medical education to have the impact that is so desperately needed, we need to get to the point where ‘active’ learning becomes our baseline educational expectation. Our research has demonstrated that learners acknowledge this very idea – if a learner is not taking notes, setting reminders to drive reflection, searching in real time to answer new questions, AND connecting to other learners (either explicitly or tacitly), then learning is ‘hit or miss at best’. When it comes to active learning strategies, we all need to ensure that our educational programs, at a very minimum, support these four ‘natural learning actions.’
Brian McGowan, PhD is the co-founder and chief learning officer at ArcheMedX, a healthcare informatics and e-learning technology company specializing in medical education. He is a research scientist and educational technologist and led Pfizer’s Medical Education Group and previously served in educational leadership roles at HealthAnswers, Inc.; Acumentis, LLC.; Cephalon; and Wyeth. He taught graduate medical education programs at Arcadia University for 10 years.
AOSpine
www.aospine.org | education@aospine.org
Copyright © 2014 AO Foundation. All rights reserved.
