There are significant differences in surgeon education in different parts of the world, even between countries with similar economies. To Franziska Schmidt these variations became reality when she moved from her native Germany to the US for an AO Spine research fellowship.
Curious as she was, and with a little help from the AO, she went on to find out more.
Here, Schmidt shares her thoughts on surgeon education, creating successful teams in hospitals for best patient outcomes, and some of her personal goals.
I wanted to treat seriously ill patients: to accompany patients in a serious period of their life, gives back a lot. It is wonderful to see symptoms disappear after surgery, for example, when a person with a foot drop can walk or drive a car again, and their pain is gone. I am grateful that I can work in this field.
My AO Spine journey started with a research fellowship at Weill Cornell in New York. I was very lucky to be able to spend almost two years with Dr. Roger Härtl and his team studying MISS. I still benefit from the experience in my clinical work here in Innsbruck, Austria, in the neurosurgical department.
When I moved to New York everything felt so different. The spectrum of the job was very different from what I had known so far. In the beginning, it seemed to me that the education was very different—not worse—just different.
In my opinion, it is the patient who suffers if the education is lacking at any point. At first, I felt everything in the US was better in terms of training, education, mentoring, and caseload. It is that caseload that makes your experience. Also, the hierarchies were flatter. But with time you realize, some things were better where I came from.
"In the end, it is the patient who suffers if the education is lacking at any point."
In most fields there is inequality in education. To find out what the differences are and to understand what we could do about them, I decided to collect data, ask as many people as possible. Maybe we could find the best of both worlds and meet somewhere in the middle. My study is basically a big PISA study for grown-ups.
At the Global Spine Congress 2019 in Toronto, I approached the AO Spine team at their booth. They put me in contact with the AO Education Institute. Michael Cunningham and Monica Ghidinelli helped me a lot with the surveys, the email blasts, and the statistics.
The AO Spine network was instrumental for the study to succeed. We received full questionnaires from almost 400 spine surgeons, both ortho and neuro. We compared the regions and the countries within North America and Europe. I am finalizing the statistical analysis and expect to publish results very soon.
We need to introduce standardized curricula and checkpoints to assure quality, like you have in school. Not only for the residents, but also for the hospitals. The AO Spine Curriculum and the AO Spine MISS Curriculum are good examples of working standards.
"We need to introduce standardized curricula and checkpoints to assure quality."
The curriculum tells you what you should be able to do at certain stages of your career and you should be able to get this from your institution.
But the most important thing in your training is to find a good and honest mentor. And to get yourself out of your comfort zone because we don’t know what we don’t know!
"The most important thing in your training is to find a good and honest mentor."
Ideally, a surgeon's learning pathway should go from simple to complex in a one-to-one teaching setting. For example, the first case is done by the attending surgeon and the second case by the resident followed by a quick feedback.
I have two attendings with a lot of clinical experience who are my surgical role models. How they approach problems and make decisions is smart. You work with them, you are on call with them, you scrub with them. That is how I find mentors, through work. Importantly, they are not criticizing you because they are grumpy, but because they actually want to improve something.
Adaption to new technologies is definitely coming rapidly, but we need better bonding to industry. I am lucky because I have good personal contacts and we talk a lot about latest improvements.
But especially for younger surgeons it is difficult to know what is out there, because you are in your own hospital bubble. You may see new innovations at conferences, but how else do you get to know what the industry is developing, unless your boss is very keen on trying new things?
New ideas in hospitals will always come through the surgeons. The hospital management usually have a background in law, economics, or business. It is very unlikely that somebody who is focusing on running the business, says, "oh, okay, please use that new technology, let's try it out and see if it works."
"New ideas in hospitals will always come through the surgeons."
Unless there is a situation like the pandemic. It literally had an impact on every person on this planet, and as always in life, there are pros and cons. We very quickly understood that, with some creativity, remote education is possible and works. And, on the other hand, I will value courses, conferences, and face-to-face discussions more than ever. I realized we cannot take anything for granted.
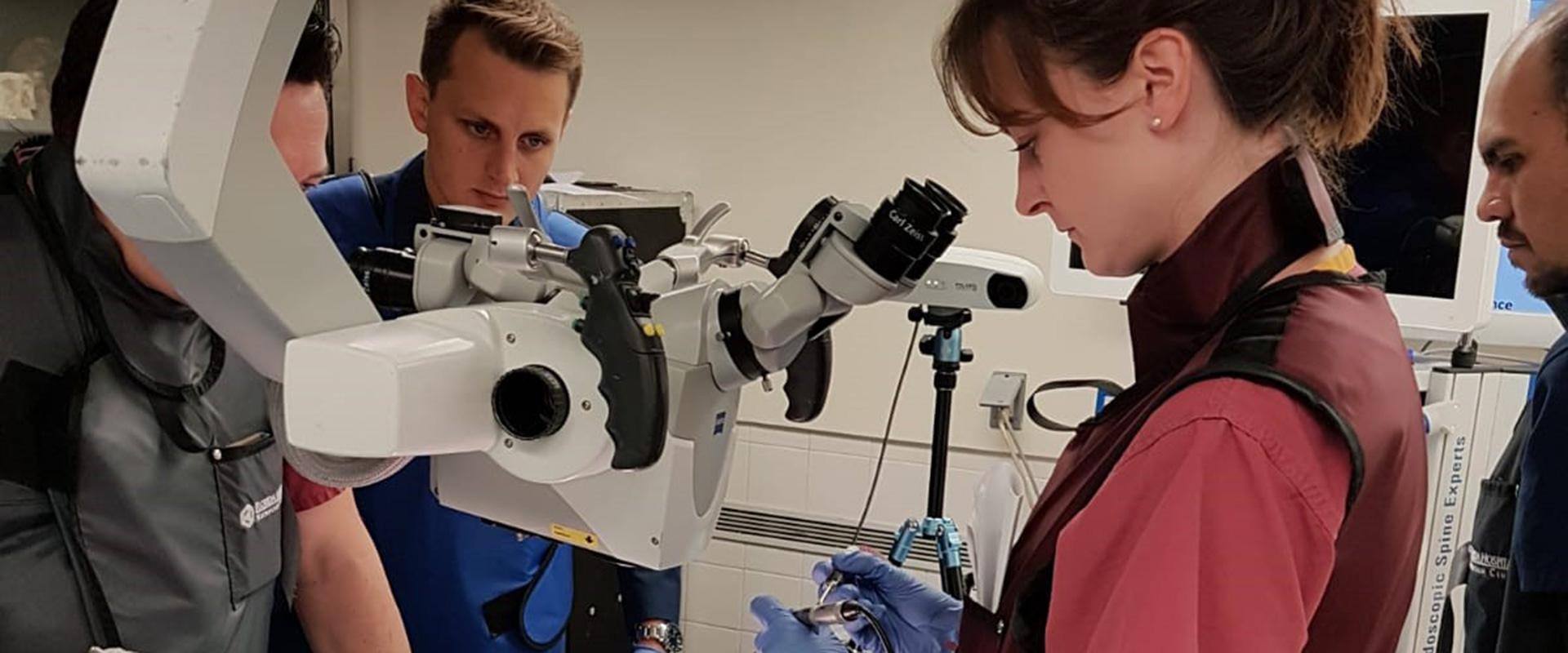
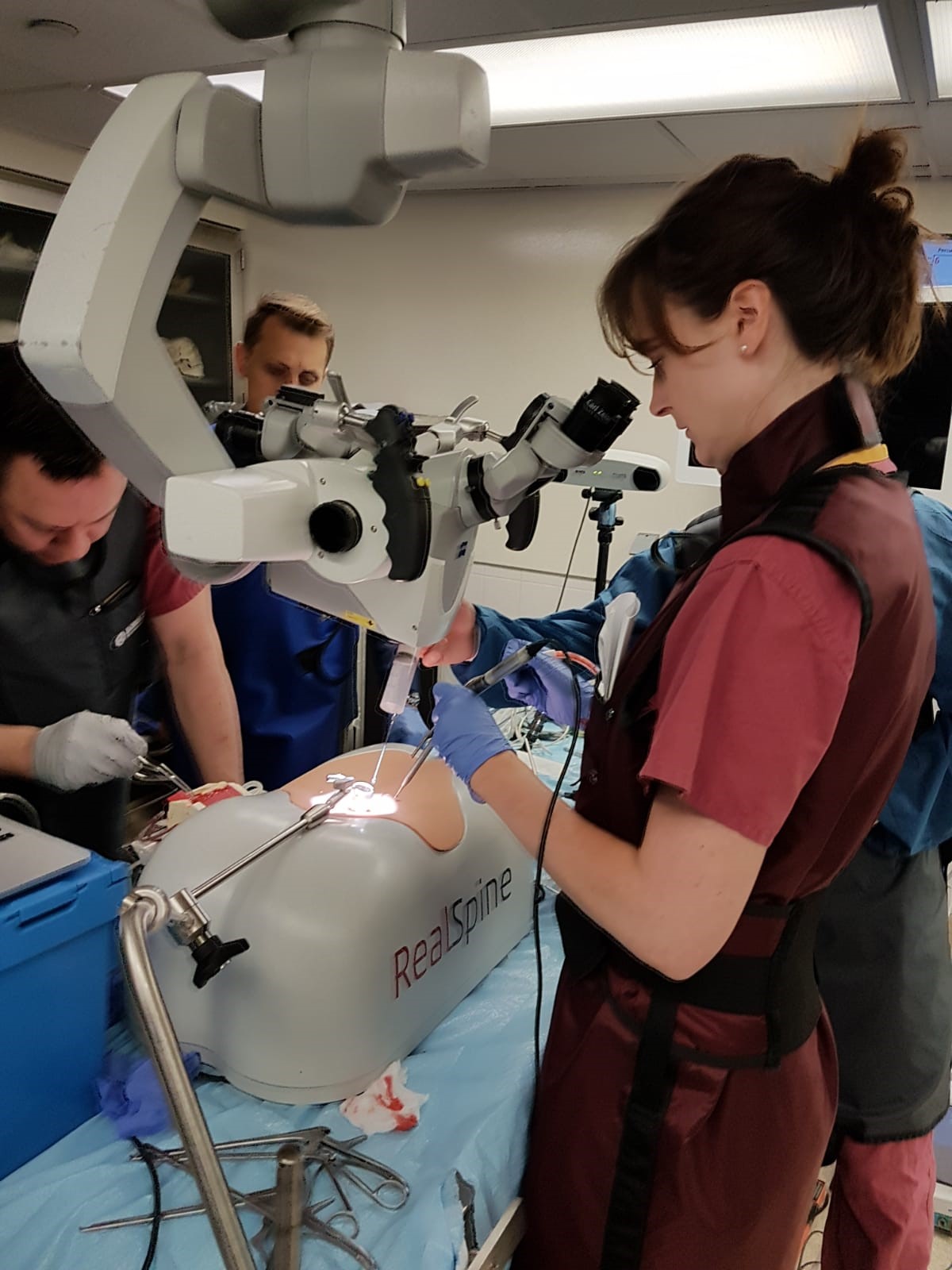
I have always been interested in education and how to improve it for residents. That is how we came up with the research questions, what can we do better in education, and is it helpful for young surgeons to superimpose anatomical structures to the microscope.
We want to understand whether AR brings a benefit to surgical education. The teams of my former boss, Roger Härtl in New York, and my current boss, Claudius Thomé in Innsbruck, Austria, are both involved.
AR is still in its infancy. Sometimes, I have the feeling that we don’t know where to put it and what to do with it. So, it is interesting to experiment and experience different attempts. The innovations will come in combination with navigation and with machine learning. But we will have to wait for the results until after the pandemic.
Nothing is more satisfying than to see your own development, and my plan is to keep on developing. Maybe I will do another AO Fellowship.
I believe everybody always brings something to the table and that the youth matters. The COVID-19 vaccination development taught us that team play is crucial in difficult situations. For example, researchers from 60 countries were working for the Biontech vaccine. This is a striking argument—diversity will always be more successful.
"Diversity will always be more successful."
We must keep in mind that also in the hospital, the team is the key. You cannot do fancy surgery with fancy technology if you do not have the physiotherapists who will walk stairs with patients afterwards, it's counterproductive. Everyone in the team is really important.
I find it empowering to see the engagement of employees in start-ups. Teams and employees are the secret for success! Companies with a flat hierarchy and high employee bonding can turn into great success stories. Maybe the hospital world could adjust towards that direction a bit more in the future.

• Franziska Schmidt is a Resident physician specializing in neurosurgery at the Medical University of Innsbruck in Austria.
• Schmidt studied medicine at the Medical University of Innsbruck. She spent one semester at the Linköping University in Sweden as an exchange student. Her specialization further took her to University Hospital Zürich in Switzerland, to Yale Medical School and to UC San Diego School of Medicine in the USA.
• After her successful doctoral dissertation in 2015, Schmidt participated in an AO Spine North America Fellowship Program, where she studied MISS with Dr. Roger Härtl (Weill Cornell, New York 2018–2020).
• Schmidt has conducted a study on regional variations in Neurosurgeons' training which will be submitted for publication this year (2021). She recently received a Research Grant from the AO Technical Commission Spine to investigate the role of Augmented Reality as an Educational Tool in MIS TLIF.
• For Schmidt, medicine is a career of choice, a second profession after a degree and having worked in Business.