
Managing spine surgery complications
All spine surgeons encounter complications in their daily practice. How we handle them dictates success rates. Minimizing risks and thinking through complication management strategies preoperatively help to create better outcomes for the surgeon and for the patient.
Complications during spine surgery are, to some degree, unavoidable and cost patients and surgeons money, time, resources, and quality of life. Minimizing complications to the greatest extent possible benefits all parties. Spine surgeons, neurosurgeons and orthopedic surgeons in general have higher rates of exposure to litigation than almost all other surgical specialties and there are particularly high rates of claims against spine surgeons [1]. Studies using various classifications of complications have reported rates of complications ranging from less than 1% to 70% [2], although the most comprehensive studies agree that the overall complication rate is about 15%2.
Definition of complications
Despite the universal agreement that complications are inevitable, there has been very little consensus on the specific definition of a complication. In his seminal textbook on spine surgery [3], Edward Benzel MD, Chairman of the Department of Neurosurgery at Cleveland Clinic and Professor of Surgery at Case Western Reserve University, in Cleveland, USA writes: “Complications must be defined to the best of our ability, avoided when possible, and aggressively managed when they occur”. Adequate preoperative planning on how to manage complications if they arise is a key element to success.
Surgical site infections
Surgical site infections are one of the most common complications of spine surgery. Rate of occurrence ranges from 0-10% [4] depending on the type of procedure. A four year review by the Scoliosis Research Society of their morbidity and mortality database found an infection rate of 2.1% based on 108,419 procedures [5]. Edward Benzel notes that, “the most common approaches in which [surgical site infections] are seen are dorsal laminectomy approaches. Infections occur at a greater frequency with dorsal approaches due to the extent of dissection and disruption of tissue planes”. Other risk factors for surgical site infections include diabetes mellitus, obesity, use of implants, and revision surgery or previous surgical site infection.
Management of both deep and superficial surgical site infections includes debridement, drainage, and antibiotics. Most often instrumentation can be retained. Prevention measures using prophylactic antibiotic administered within 60 minutes of skin incision and monitoring of serum glucose levels (pre and postoperatively) have also proven effective [4].
Dural tears
Incidental dural tears are another common complication of spine surgery. As with surgical site infections, a posterior approach and revision surgery increases the risks for dural tears, especially if there is epidural scarring. Some studies have found that advanced patient age is also associated with an increased risk of dural tears [6]. While rates of dural tears are usually low (1-4%, with a few studies >10%), small tears with no obvious cerebrospinal fluid leakage can be difficult to visualize during surgery.
Intraoperative repairs of dural tears includes: fibrin glue, sutures, and muscle and fascial graft. Dural tears that are not identified intraoperatively or not fully repaired can lead to sepsis, meningocele, persistent cerebrospinal fluid leak, and hematoma. Postoperative management can include revision procedures and conservative treatment.
Other common complications
Some common complications of spine surgery relate more specifically to spinal segment and the type of surgery performed. For instance, esophageal injuries (including dysphagia and dysphonia) are common in cervical surgeries, however, symptoms are usually short-lived and mild. A review of complications in spine surgery [4] found that:
Thoracolumbar complications were more often related to the procedure performed, with routine reports of pseudarthrosis and hardware failures. Commonly reported thoracolumbar complications also included postoperative radiculopathies, wound infections, and urinary tract infections. Cervical complications were more often approach related, including dysphagia and dysphonia. Other common cervical complications included postoperative hematoma, C-5 nerve root palsy, increase in axial neck pain, and hardware failures. Thoracolumbar complications were more often related to the procedure performed, with routine reports of pseudarthrosis and hardware failures. Commonly reported thoracolumbar complications also included postoperative radiculopathies, wound infections, and urinary tract infections. Cervical complications were more often approach related, including dysphagia and dysphonia. Other common cervical complications included postoperative hematoma, C-5 nerve root palsy, increase in axial neck pain, and hardware failures.
Complications associated with implants usually stem from either implant positioning or failure of fixation of the implant. In either case revision surgery is often needed. Preoperative evaluation of vascular and intraoperative fluoroscopy and computer imaging can help avoid complications.
Implementing outcome metrics
The importance of good patient and procedure selection techniques cannot be underestimated. Some have asserted that high procedure rates in particular geographical areas may indicate that patient and procedure selection are not being optimized. Edward Benzel believes that this is a substantial problem,
“We need to develop and implement appropriate outcome metrics and measures so that we can reward those surgeons who have good outcomes (high value = quality/cost). Spine surgery for pain is a precarious undertaking. Outcomes are, in general, poor – resulting in more surgery and chronic pain syndrome. It is difficult to ‘fix’ these patients with more surgery.”
It has even been suggested that reducing the number of unnecessary spine surgeries would have a greater impact on complication rates than focusing on optimizing the technical aspects of the surgeries that are performed.
The patient’s perspective
Looking at things from the patient perspective can also be useful when working to create better outcomes and avoid complications. What constitutes a “complication” may be very different from a patient versus surgeon perspective.
One study found that patients who perceived there to be complications were overall less satisfied with the outcome of their surgery. Likewise, certain occurrences that a surgeon would unquestionably classify as a complication (such as a dural tear) were insignificant to the patient if treated without the need for postoperative intervention.
How to manage complications
Adequate preoperative planning and being mentally prepared can make a significant difference when intraoperative complications occur. Edward Benzel suggests three tips for mentally managing intraoperative complications:
- Do not panic, be calm and hopefully you anticipated that such a problem could occur. A preplanned solution to an intraoperatively encountered complication makes everything smoother and safer.
- Do not hurry. Mistakes can only be compounded by abrupt and aggressive maneuvers that are often used in response to a complication.
- The surgeon must be honest with herself/himself. Ask this question – “what would I want done if I were the patient?”
Combining technical and nontechnical techniques and training can help avoid complications and create the better outcomes for patients. Complications are inevitable and how we manage them dictates success rates.
References
- CL Taylor (2014) Neurosurgical practice liability: relative risk by procedure type. Neurosurgery Aug 25.
- R Nasser (2010) Complications in spine surgery. J. Neurosrug. Spine 13:144-157.
- E Benzel (2012) Spine Surgery, 2 Volume Set: Techniques, Complication Avoidance and Management. 3rd edition. Elsevier, Philadelphia, PA. 2248pgs.
- D Gloystein et al (2010) Complications of Spine Surgery: Surgical Site Infections. Orthopaedic Knowledge Online 8(7).
- JS Smith et al (2011) Rates of Infection After Spine Surgery Based on 108,419 Procedures. Spine 36(7)556-563.
- BJ Williams et al (2011) Incidence of Unintended Durotomy in Spine Surgery based on 108,478 cases. Neurosurgery 68(1)117-124.
- D Grob, AF Mannion (2009) The Patient’s Perspective on Complications After Spine Surgery. Eur. Spine J. 18(3)S380-S385
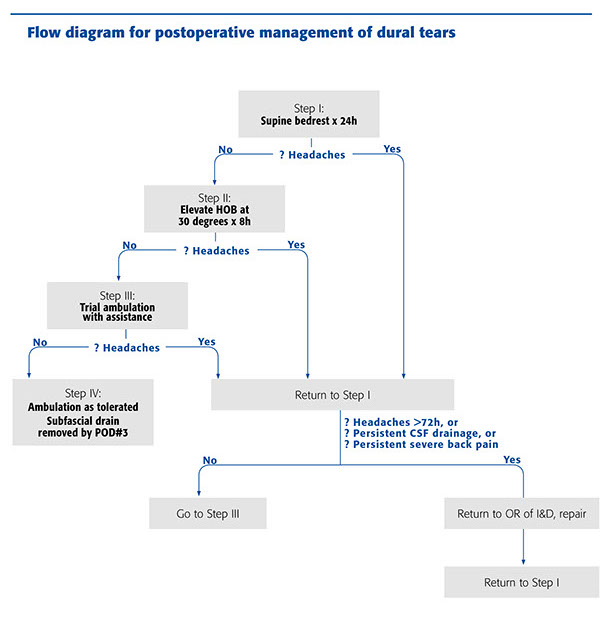
Flow diagram for postoperative management of dural tears
Source: Postoperative Management Protocol for Incidental Dural Tears During Degenerative Lumbar Spine Surgery (Khan et al)
This contribution and article represent the opinion of the individual writer exclusively and not necessarily the opinion of AOSpine.
AOSpine
www.aospine.org | membership@aospine.org
Copyright © 2014 AO Foundation. All rights reserved.
