
![]() Back to contents
Back to contents
How to improve doctor-patient communication
Interpersonal communication is often regarded as a “soft skill” in healthcare, but it constitutes a primary ingredient for effective treatment and better patient outcomes.

Does this sound familiar? You are a busy spine surgeon who has diagnoses to make, operations to perform, records to enter, targets to meet, budgets to balance and, after all that, you have little time for long conversations with your patients.
For a long time many doctors didn’t realize how badly these pressures impacted their patients' wellbeing. In 1998, a national survey conducted by American Academy of Orthopaedic Surgeons revealed that its members were rated “high tech – low touch” [1]. What’s more, the extreme disparity between how doctors saw themselves versus how their patients rated them rang alarm bells. Whereas 75% of surgeons thought they had communicated well with their patients, only 21% of their clients agreed [2].
As it turns out, much more than public image was at stake in this sort of misunderstanding.
Table I: Discrepancies between AAOS members' self-assessment and patient's perceptions of orthopedic care
| Physician's perception: I believe patients view me as: | Patient's perception | |
|---|---|---|
| Highly trained | 70% | 64% |
| Having successful results | 64% | 53% |
| Being caring and compassionate | 71% | 37% |
| Spending time with patients | 71% | 36% |
| Providing valuable service | 65% | 35% |
Courtesy of John Tongue, MD and AAOS
Patient complaints
Most complaints about doctors [4] concern communication issues. Indeed, studies [5-8] show that doctors involved in malpractice cases share certain traits. Their consultation times are shorter than average (15 minutes versus the average which is closer to 20 minutes); they spend less time orienting patients towards what to expect during treatment; they rarely, if ever, consult with patients about their health care preferences, nor check for understanding of diagnosis and prescribed treatment strategies. They also fail to disclose medical errors.
Doctors might sometimes blame bad outcomes on the patients themselves who failed to follow their treatment plan, but as it turns out compliance is also tied to the doctor’s ability to communicate the plan in the first place. A 2009 meta-review of more than 100 published cases found that non-adherence was 19% more likely if doctors failed to collaborate with their patients and clarify the requirements [9]. Yet, if those same doctors received communication skills training their patients were 12% more likely to seek follow-up consultations and comply with their treatment plan.
Malpractice Claims
Communication breakdown is most often cited as the reason that patients decide to sue their orthopedic surgeon.
71%
Poor relationship
32%
Patient felt deserted
26%
Patient felt information was poorly delivered
29%
Patient felt devalued
Confusion reigns:
Without adequate communication procedures in place:
62% of hospitalized patients do not understand their treatment plan [4].
After discharge, “less than half of patients are able to list their diagnoses, the name(s) of their medication(s), their purpose, or the major side effect(s)”.
Between 25-50% of patient do not follow through on their treatment plans.
Training clarifies:
Better communication skills can help people get better, faster:
Patients are 19% more likely to forego their treatment plan if doctors communicate poorly by failing to consult with them and clarifying the requirements [6].
Yet, if those same doctors receive communication skills training their patients are 12%more likely to commit to the agreed treatment.
Source: AAOS

Make your patients heal faster
A common theme throughout these studies is that if patients feel respected and cared for by their doctor they are more likely to heal [10]. That is, they are more likely to commit to their own recovery, rather than stew over grievances and complain about problems. They are also more likely to forgive mistakes and work to overcome setbacks. On the other hand, if patients feel brutalized, confused, or alienated by their encounter with the medical profession they are more likely to sue.
| Table II Contribution of communication breakdowns to malpractice risks | |
|---|---|
| Patient mentioning poor relationship as reason for claim | 71% |
| Patient felt deserted | 32% |
| Patient felt devalued | 29% |
| Patient felt information delivered poorly | 26% |
| Patient felt there was a lack of understanding by the clinician | 13% |
Courtesy of John Tongue, MD and AAOS
The brilliant, but infamously callous Dr Gregory House in the popular drama series House might be entertaining on television, but in reality is his professional brilliance worth all that much? If you answered no you’re not alone. A Harris Interactive(R) poll of 2,267 US adults conducted online during September 2004 for the Wall Street Journal found that the number of patients who valued their doctor’s interpersonal skills (85%) outnumbered those who cared about their medical judgment (80%). Many admitted that they had changed doctors for this very reason.
"These startling numbers show that doctors' training and knowledge of new medical treatments to many patients is less important than their interpersonal skills -- treating patients with respect, listening carefully, being easy to talk to, taking patients' concerns seriously, spending enough time with them, and really caring," says Humphrey Taylor, chairman of The Harris Poll(R) [11].
Good patient/physician relationships are the magic ingredient of health care. They help to offset the emotional ups and downs of illness. By facilitating the ready flow of information and providing much needed psychological support, a collaborative doctor patient relationship also encourages a sense of empowerment. This can promote an early recovery and can also help to ensure that unnecessary hospital re-admissions are less likely to occur [13].
Doctors sometimes complain that they feel like
vending machines, rather than trusted advisors [14].
These teaching videos compare what can go wrong in the consultation room as opposed to what happens when doctors are trained to communicate more effectively.
A realistic portrayal of a medical consultation gone wrong.
Ways to better manage such situations
Steps to take
Patient-centered care emphasizes that patients are whole people rather than mere body parts. It also aims to include them as active partners within their own treatment. This approach characterized the American Academy of Orthopaedic Surgeon’s (AAOS) response to that alarming 1998 discovery that their member's communication skills needed an industry wide overhaul. In partnership with Bayer Institute for Health Care Communication (BIHCC) the AAOS developed a communication skills mentorship program based upon an education model known as the “4Es” (engage, empathize, educate, enlist).
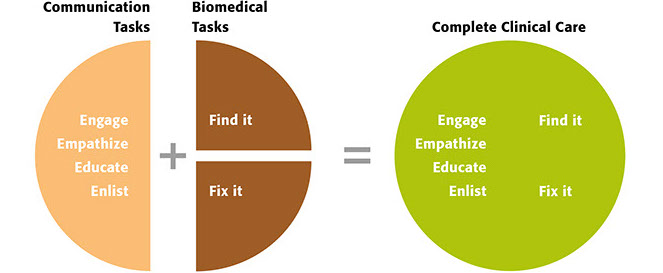
The "4Es" define the communication tasks, combined with traditionally taught biomedical tasks, that are necessary for complete clinical care.
Courtesy of John Tongue, MD and AAOS
By combining communication skills with clinical care the program models a practical approach to patient-centered care.
6 ways to build good physician/patient relationships
1) Listen
Patients often shut down in the face of a dominant doctor, if they’re not interrupted first. Studies show that most patients are likely to be interrupted after speaking for just twenty-three seconds [15, 16]. Less than 25% of patients ever get to complete their initial thoughts. Physicians all too easily make assumptions that turn out to be incorrect [17].
A good technique to counter this tendency is to ask open-ended questions, such as “What can I do for you today?” Give patients at least two minutes to answer.
Patients can also ask their own questions. Associate Professor in clinical medicine at the University of California, Dr. Gurpreet Dhaliwal recommends these prompts [18]:
• Idea—What is your idea about what is going on?
• Concerns—What are you most worried about?
• Expectations—What do you expect me to be able to do?
2) Consult, rather than control
Check patients’ expectations and concerns. Explain your understanding of the situation whilst endeavoring to accommodate theirs. Compliance is more likely if you both can come to a mutual understanding. After informing patients about the various treatment options available to them and what they might reasonably expect “check in” questions might be “How important do you think it is to do these things?” and “How confident are you that you can do these things?”.
To engage your patients more actively in their own recovery you might also say something like “When you return, I’ll ask you if you are better. And if you are better I’ll ask you how much better – 10%, 50%, 90%? So be thinking about this until I see you then”.
3) Sound concerned, rather than dominant
With no prior knowledge of a doctor’s history trained analysts can accurately predict malpractice targets just from their tone of voice [6]. It is important to ask open-ended questions using a positive tone and reassure patients about their fears.
4) Appear interested and try to be available
Smile when they arrive, sit down during consultations and attend to patient comfort. Show attention by nodding your head and maintaining eye contact. Even if you aren’t available 24/7, ensure that emergency contacts are on hand if required.
5) Laugh
Doctors targeted for malpractice suits rarely laugh. Of course, it helps to be sensitive to the situation involved and be careful that humor is not misconstrued as derision. Nevertheless, shared laughter can foster a sense of camaraderie.
6) Be positive and keep patients informed
In their guide to patient-centered care the AAOS recommends full disclosure of medical errors. Tips to do so include putting aside a designated time and space for the discussion free from external interruptions. Explain the situation in detail using clear language and an empathetic tone. Check in regularly for understanding and acknowledge the likely emotional reactions with summary statements that show you hear what they are saying and appreciate their pain. Statements such as “We are sorry that this has happened to you” demonstrate empathy without necessarily accepting blame.
It is important to be honest with patients, but also offer psychological support. When an appointment concludes it helps to look patients in the eye and shake their hands, whilst expressing your hopes for the future. This can give patients something to hold on to.
Keys to successful patient communication
Don’t say this
Say this instead
Please read and sign this informed consent form for your surgery
There are risks and complications that can happen with this surgery that you will read about in this material. Tell me what questions you have.
Do you understand the treatment plan we just discussed?
Please repeat back to me in your own words the treatment plan we just discussed
I know how you feel about your trauma injury. I’ve been a trauma specialist for 30 years.
I know this is a very difficult time for you and your family. Let me help you get through this by answering as many questions as you need to ask.
Your appointment today is about your spinal surgery, so we can’t talk about your knee pain. That will have to wait until another appointment
I want to make sure that I know about the pain you're feeling in your spine as well as your knee since one can affect the other.
They are making me use this laptop with all my patients, and I can’t find anything on it!
Our practice is using a new computer system, so I will be typing what you tell me as we talk. Please let me know if I fail to answer one of your questions.
Do you understand how to take this medication?
To make sure I have explained everything, please repeat back to me what I said about this medication.
I don’t believe in alternative medicines. It’s hocus pocus. You have to stay on your current prescriptions.
What questions do you have about alternative medicines? I will research your questions and get back to you within the week. In the meantime, will you agree to continue your current prescriptions?
Source: The Doctors Co.
Eyes on the bottom line
Unfortunately with profits linked to patient numbers and satisfactory turnover rates, the health care industry is all too often geared towards quantity, rather than quality care.
Dr David Forster, an executive co-producer of the House series is matter of fact about this: “If you want doctors to improve communication skills with patients, then pay them for their time to do it. Doctors are very good at figuring out what the system rewards. The system financially rewards ‘doing things’… ie. prescribing and procedures. So, not surprisingly, that's what doctors do well” [19].
Yet, as the 1999 report To Err Is Human [20] highlighted, rewards that might encourage shortcuts can also be deadly. Follow up studies point to communication breakdown as the main cause of an alarming number of life and death mishaps [21].
The “DUN” Factors
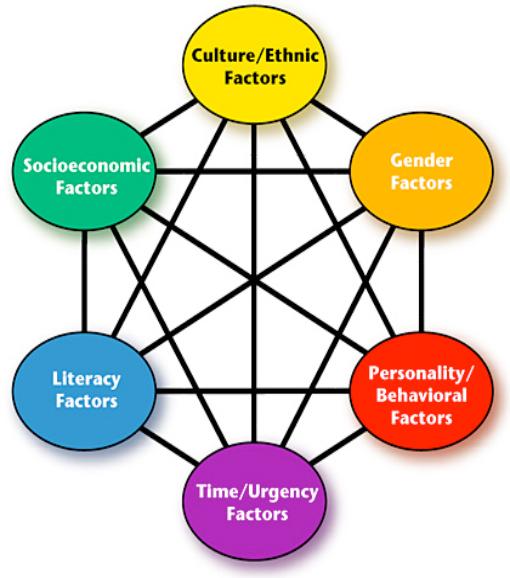 Medical consultant and author Michael Woods MD calls these sorts of complications “DUN” Factors, the “Dynamic, Unpredictable and Non-Linear” curve-balls that characterize “life as it really is” [24].
Medical consultant and author Michael Woods MD calls these sorts of complications “DUN” Factors, the “Dynamic, Unpredictable and Non-Linear” curve-balls that characterize “life as it really is” [24].
Woods identifies at least 6 types of real world challenges that can seriously compromise communication efforts:
1. Cultural/Ethnic
According to some cultural beliefs, for example, telling patients that certain procedures involve risks increases the likelihood of an adverse outcome.
2. Socioeconomic
Doctors might assume that patients from lower socioeconomic circumstances desire less information, but this is a dangerous assumption.
3. Gender
Sadly, male physicians are more likely to overestimate their communication skills and under-value the role of interpersonal rapport within their own practice. As a result they are three times more likely to be involved in malpractice suits.
4. Literacy
Large number of patients with English as a second language may not be able to understand written instructions.
5. Personality/Behavioral Issues
Physicians with behavioral issues such as the tendency to yell, intimidate, condescend or abuse their patients and co-workers are a liability risk.
6. Time/Urgency
Hectic schedules produce fatigue. “Tired people are less patient, more error-prone, and reduce the willingness of even the most altruistic individual to spend the time needed to communicate effectively”.
The Six Factors of Communication Risk (click to zoom).
Image courtesy of Patient Safety & Quality Healthcare [24]
A team approach
These sorts of challenges can’t be solved individually. They often require a team response that can support the patient- physician relationship. For instance, assistants could help with digital record entry, or the medical interview load could be more productively shared with a nurse, psychologist, or translator. These alternatives offer a lot of promise both for patients and health care providers, but in order to be truly viable the particular challenges of working in teams also need to be addressed:
- It’s estimated that at least 80% of medical errors involve miscommunication between caregivers when patients are transferred or handed over [25].
- Patient mortality rates climb when staff working in intensive care units fail to collaborate [26].
Patient safety experts warn about the dangers of strict work hierarchies.
Currently doctors and nurses are trained to use different words to describe the same events. Some commentators argue that common ground needs to be built in to medical training from the start [27].
One nurses’ sobering account of a communication breakdown in an operating theatre.
Intra-team communication skills training is vital.
These teaching videos model techniques to help address a few of the more common communication issues.
Intra-staff communication ends badly when a consultant yells at a resident.
A more empathetic communication style helps to avoid this sort of unnecessary conflict.
Can social media tools help?
These days, patients might reasonably expect an immediate response to their questions 24/7 via digital networking tools such as emails, text messages and twitter. But can reliable and caring medical treatment be reduced to a tweet?
Doctors are divided. Only 21% of patients can access their doctors via email, for example, despite the fact that those who do generally find this service beneficial [28].
Some social media tools are helpful nevertheless. Online networks, for instance, have become important support sites for patients. Doctors could work more closely with these communities. Some believe that online forums, Facebook and twitter are ideal dissemination points for patient education materials. At the same time they urge physicians to monitor these sites for reports of new diseases and infections [29].
Fred Hassan, chairman of Bausch and Lomb nevertheless warns that iPad can’t fix everything. “Brochures and iPad help with communication, but empathy is still the decisive key”[30].
 “The doctor-patient relationship is being more and more marginalized.”
“The doctor-patient relationship is being more and more marginalized.”
Co-founder of AOSpine and UK consultant spine surgeon John O’Dowd shares his view on the future of doctor-patient communication.
How does the doctor-patient relationship impact outcomes?
Communication within the doctor-patient relationship is critical to outcomes. Spine surgeons have to be quick relationship builders; we just have minutes to build enough trust for a patient to consent to an operation. Additionally, spine surgeons benefit when they have a good reputation or a patient is recommended by someone they know. In these cases patients show up to a consultation with a degree of trust already established. Listening is critical, especially since surgeons may meet their patients only once.
Do you provide additional information outside the doctor-patient exchange?
It is important to not overload a patient with too much information during a meeting. Focus on the most important points, answer all their questions and direct them to an information portal – website, brochures, and/or videos. I encourage patients to record our meetings on their mobile phones so they can listen to them again at a later time. Increasingly surgeons only see their patients once and the more detailed preoperative counselling is done by non-medical healthcare professionals. The spine surgeon community has made available online high quality information over the past 10 years, to the benefit of everyone. Patients with access to high quality, accurate information have much more insight into what they are undergoing.
How do you see doctor-patient communication evolving?
The doctor-patient relationship is being more and more marginalized in modern healthcare and may become irrelevant within our working lifetime. Cost and effectiveness are the bottom lines and healthcare interactions are changing from a doctor-patient interaction to one between a citizen and the state (or insurance company). Healthcare is becoming algorithm, pathway and guideline driven with much less focus on face-to-face interactions.
Is how we measure quality in healthcare also changing?
The quality of healthcare is increasingly being measured by the quality of a patient's interaction with the system. Patients are asked, “Would you recommend this hospital?” and then told to push a red or green button to indicate their happiness or displeasure. This is madness to me. The quality of a healthcare intervention should be based more on meaningful and relevant clinical outcomes- not if a doctor has been nice to you. For some reason there is an obsession in Anglophone countries with doctors being nice to patients and being good communicators. I think we have to be careful and ask “why this is?” Is it so people can have a green button experience or because it improves the quality of the healthcare interaction?
Statistics show that patients who pursue malpractice lawsuits often state poor communication from their doctor as one of the reasons.
I am cynical about this type of evidence. Of course some doctors are poor communicators and this can trigger complaints, especially if something goes wrong with the surgical procedure. However there is a default position in the medical malpractice world to say that the doctor didn’t say the right things, but we have to be careful about this. Whilst there is varied quality of consultations, there is often a transmit and receive issue. Some patients do not hear what the doctor is saying. Some think they know everything before coming and don’t listen. Doctors are trained to be good listeners; patients are often poor listeners, and can be poor at retaining information.
How do communication skills come into play when something goes wrong during a procedure?
When something goes wrong with a surgical treatment I think what the patient needs is for the doctor to keep their cool and not lose their nerve. Inexperienced surgeons panic, become distressed and stressed, because they don’t know what to do. The patient sees this and it leads to a very rapid decline in the relationship. Surgeons need to understand that they have to be able to cope in the same way an aircraft pilot would when something goes wrong. This is where surgical safety courses are very beneficial. We can take people through bad scenarios and help them see how they would respond.
What should be done to improve doctor patient communication?
If you accept that communication is important, both sides have to be trained and taught to communicate better. There is a role here for the medical schools, and of course AOSpine offers courses as part of the Faculty Education Program that delve into the non-verbal challenges of communication. But patients also need to be taught to communicate better too. Particularly in the UK, where health literacy is low, we need to help citizens understand the importance of healthcare issues and to help them to assimilate and process healthcare information. There are always two sides to the doctor-patient relationship.
—
ABOUT John O’Dowd, FRCS Orth
A consultant orthopedic spine surgeon, with a private practice based in London and a health service practice based in Hampshire. John is founder and medical director of the RealHealth Institute in the UK and the Netherlands. Recent ex-president of the Society for Back Pain Research, a reviewer for a number of high profile spine journals, he was one of the founders of AOSpine and has lectured on and chaired courses for AOSpine around the world.
REFERENCES
1. American Academy of Orthopaedic Surgeons, Public Image Investigation. 1998.
2. Canale ST., How the orthopaedist believes he is perceived by the public and how the public actually perceives the orthopaedist., in AAOS Symposium, Patient-Physician Communication. Presented at the Annual Meeting of the American Association of Orthopaedic Surgeons. 2000 Mar 15 - 18: Orlando, Fl.
3. Tongue, J.R., H.R. Epps, and L.L. Forese, Communication Skills for Patient-Centered CareResearch-Based, Easily Learned Techniques for Medical Interviews That Benefit Orthopaedic Surgeons and Their Patients. The Journal of Bone & Joint Surgery, 2005. 87(3): p. 652-658.
4. Landro, L. The Talking Cure for Health Care: Improving the ways doctors communicate with their patients can lead to better care—and lower costs. 2013 10.12.14]; Available from: HYPERLINK "http://www.wsj.com/articles/SB10001424127887323628804578346223960774296" http://www.wsj.com/articles/SB10001424127887323628804578346223960774296.
5. Levinson, W., et al., Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. Jama, 1997. 277(7): p. 553-559.
6. Ambady, N., et al., Surgeons' tone of voice: a clue to malpractice history. Surgery, 2002. 132(1): p. 5-9.
7. Beckman, H.B., et al., The doctor-patient relationship and malpractice: lessons from plaintiff depositions. Archives of Internal Medicine, 1994. 154(12): p. 1365-1370.
8. Hickson, G.B., et al., Factors that prompted families to file medical malpractice claims following perinatal injuries. Jama, 1992. 267(10): p. 1359-1363.
9. Zolnierek, K.B.H. and M.R. DiMatteo, Physician communication and patient adherence to treatment: a meta-analysis. Medical care, 2009. 47(8): p. 826.
10. Kim, S.S., S. Kaplowitz, and M.V. Johnston, The effects of physician empathy on patient satisfaction and compliance. Evaluation & the health professions, 2004. 27(3): p. 237-251.
11. The Free Library. Doctors' Interpersonal Skills Valued More Than Their Training or Being Up-to-Date. 2004 10.12.14]; Available from: HYPERLINK "http://www.thefreelibrary.com/Doctors'+Interpersonal+Skills+Valued+More+Than+Their+Training+or...-a0122712044" http://www.thefreelibrary.com/Doctors'+Interpersonal+Skills+Valued+More+Than+Their+Training+or...-a0122712044.
12. Canale, S.T., Falling in Love Again*. The Journal of Bone & Joint Surgery, 2000. 82(5): p. 739-739.
13. Ha, J.F. and N. Longnecker, Doctor-patient communication: a review. The Ochsner Journal, 2010. 10(1): p. 38-43.
14. Daniel J Denoon. Getting The Care You Need: Can We Talk? 2001 10.12.13]; Available from: HYPERLINK "http://www.webmd.com/a-to-z-guides/features/getting-care-you-need-feature" http://www.webmd.com/a-to-z-guides/features/getting-care-you-need-feature.
15. Beckman, H.B. and R.M. Frankel, The effect of physician behavior on the collection of data. Annals of Internal medicine, 1984. 101(5): p. 692-696.
16. Marvel, M.K., et al., Soliciting the patient's agenda: have we improved? Jama, 1999. 281(3): p. 283-287.
17. Healthcare, P.S.Q. The DUN Factor: The Six Factors of Communication Risk. 2014 10.12.14]; Available from: HYPERLINK "http://psqh.com/the-dun-factor-the-six-factors-of-communication-risk?highlight=WyJjb21tdW5pY2F0aW9uIiwic2tpbGxzIiwiY29tbXVuaWNhdGlvbiBza2lsbHMiXQ==" http://psqh.com/the-dun-factor-the-six-factors-of-communication-risk?highlight=WyJjb21tdW5pY2F0aW9uIiwic2tpbGxzIiwiY29tbXVuaWNhdGlvbiBza2lsbHMiXQ==.
18. Dhaliwal, G. The Experts: How to improve Doctor-Patient Communication. 2013 10.12.14]; Available from: HYPERLINK "http://www.wsj.com/articles/SB10001424127887324050304578411251805908228" http://www.wsj.com/articles/SB10001424127887324050304578411251805908228.
19. Forster, D. The Experts: How to improve Doctor-Patient Communication. 2013 10.12.14]; Available from: HYPERLINK "http://www.wsj.com/articles/SB10001424127887324050304578411251805908228" http://www.wsj.com/articles/SB10001424127887324050304578411251805908228.
20. Kohn, L.T., J.M. Corrigan, and M.S. Donaldson, To Err Is Human:: Building a Safer Health System. Vol. 627. 2000: National Academies Press.
21. Joint Commission, N.D. Root causes event type 2004-2011. 2012 10.12.13]; Available from: HYPERLINK "http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_2004-2011.pdf" http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_2004-2011.pdf.
22. Brown, J.B., et al., Effect of Clinician Communication Skills Training on Patient SatisfactionA Randomized, Controlled Trial. Annals of Internal Medicine, 1999. 131(11): p. 822-829.
23. DiMatteo, M., The role of the physician in the emerging health care environment. Western Journal of Medicine, 1998. 168(5): p. 328.
24. Michael Woods, M., The DUN Factor: How Communication Complicates the Patient Safety Movement. 2014. 3(3): p. 40 - 44.
25. Health-Care, J.C.C.f.T. Project Detail: Hand-off Communications. 2014 10.12.14]; Available from: HYPERLINK "http://www.centerfortransforminghealthcare.org/projects/detail.aspx?Project=1" http://www.centerfortransforminghealthcare.org/projects/detail.aspx?Project=1.
26. Knaus, W.A., et al., An evaluation of outcome from intensive care in major medical centers. Annals of Internal Medicine, 1986. 104(3): p. 410-418.
27. LaBranche, B., M. Michael Parris, and S. MSIE, The Silent Treatment: Why Safety Tools and Checklists Aren’t Enough.
28. K. Stremikis, C. Schoen, and A.K. Fryer. A Call for Change: The 2011 Commonwealth Fund Survey of Public Views of the U.S. Health System. April, 2011 10.12.14]; Available from: A Call for Change: The 2011 Commonwealth Fund Survey of Public Views of the U.S. Health System.
29. J. Lester, B., et al. How Online Patient - Networks Can Enhance Quality and Reduce Errors. 2014 10.12.14]; Available from: HYPERLINK "http://psqh.com/online-patient-networks-how-online-patient-networks-can-enhance-quality-and-reduce-errors?highlight=WyJkb2N0b3IiLCJwYXRpZW50IiwicmVsYXRpb25zIiwiZG9jdG9yIHBhdGllbnQiLCJwYXRpZW50IHJlbGF0aW9ucyJd" http://psqh.com/online-patient-networks-how-online-patient-networks-can-enhance-quality-and-reduce-errors?highlight=WyJkb2N0b3IiLCJwYXRpZW50IiwicmVsYXRpb25zIiwiZG9jdG9yIHBhdGllbnQiLCJwYXRpZW50IHJlbGF0aW9ucyJd.
30. Hassan, F. The Experts: How to improve Doctor-Patient Communication. 2013 10.12.14]; Available from: HYPERLINK "http://www.wsj.com/articles/SB10001424127887324050304578411251805908228" http://www.wsj.com/articles/SB10001424127887324050304578411251805908228.
The articles published in this newsletter reflect the opinions of the writers only and not those of AOSpine
