
Jens Chapman, Marcel Dvorak, S. Rajasekaran, Lorin Benneker, Frank Kandziora, Cumhur Öner (Chairperson), Klaus Schnake, Emiliano Vialle and María Alvarez Sánchez at the AOSpine Knowledge Forum Trauma Steering Committee meeting in Singapore, May 2018
Important goal for AOSpine study defining treatment guidelines for Thoracolumbar Burst Fractures—
Eastern Europe and Middle East pacing patient recruitment
A study aimed at defining optimal treatment for thoracolumbar burst fractures in neurologically intact patients currently enrolled 117 patients, more than half the total sample needed to complete the study. A specific subgroup analysis will be performed on those cases classified with true equipoise. The AOSpine Knowledge Forum Trauma study is an example of successful research globalization and what mentorship at its best can lead to.
While burst fractures account for almost half of all thoracolumbar spine injuries, there is significant variability in care provided. “We all have experienced this”, Principal Investigator (PI) Marcel Dvorak says. “Residents or fellows often recommend treatment that we would not necessarily consider; another attending may have treated what we consider to be a “We have all experienced the variations in care provided.”surgical fracture non-operatively. Even a case discussion at an AO meeting does not always results in a real consensus.”
The controversy is fueled by studies pointing to different directions: some studies show increased patient satisfaction and positive socio-economic results with surgical treatment; others demonstrate improved outcomes and lower morbidity with non-surgical treatment.
AOSpine strives for best evidence-based care
To address the variations, the AOSpine Knowledge Forum Trauma is performing a prospective cohort analysis and investigating the clinical outcomes of treatment alternatives. The observational international multicenter study will investigate whether surgical compared to non-surgical treatment leads to a better clinical outcome during the first year after the primary treatment.
An additional analysis will look more specifically at a sub-group of patients, who—according to a blinded expert panel—would qualify for both surgical and non-surgical treatment due to “The AO is committed to collecting the evidence required to inform the best care for our patients.”clinical equipoise. In addition, a cost-effectiveness analysis will be performed to define the social impact and to measure the health economic aspects for the different treatment options. A patient diary includes the Oswestry Disability Index and employment information with an indirect costs questionnaire. The diary will continue two years after treatment and all interventions and examinations are considered as standard of care.
The study group expects to finalize patient enrolment by the end of 2019 and get the first answers in a few years.
“What we need to do is to continue to rely on our personal experience and patient preference, but to infuse this with some carefully collected prospective outcomes data that can inform our discussions and decision making”, Dvorak says. “Variation in clinical practice can be healthy, but when it occurs in the environment of a lack of objective patient-based outcomes, it can lead to over or under-treatment. The AO is committed to collecting the evidence required to inform the best care for our patients.”

 Mohammad El-Sharkawi, S. Rajasekaran, Cumhur Öner, Lorin Benneker, and Emiliano Vialle agree treatment guidelines are important for the patients to receive the best care. Guidelines have also a wider economic implication. “To get funds back, we must provide the insurers with good clinical data”, Benneker reminds.Cezar Popescu commends his neurosurgeon fellows, who invariably inform him when a patient with a thoracolumbar fracture is admitted.2 - 2<>
Mohammad El-Sharkawi, S. Rajasekaran, Cumhur Öner, Lorin Benneker, and Emiliano Vialle agree treatment guidelines are important for the patients to receive the best care. Guidelines have also a wider economic implication. “To get funds back, we must provide the insurers with good clinical data”, Benneker reminds.Cezar Popescu commends his neurosurgeon fellows, who invariably inform him when a patient with a thoracolumbar fracture is admitted.2 - 2<>
Global participation secures comprehensive sample
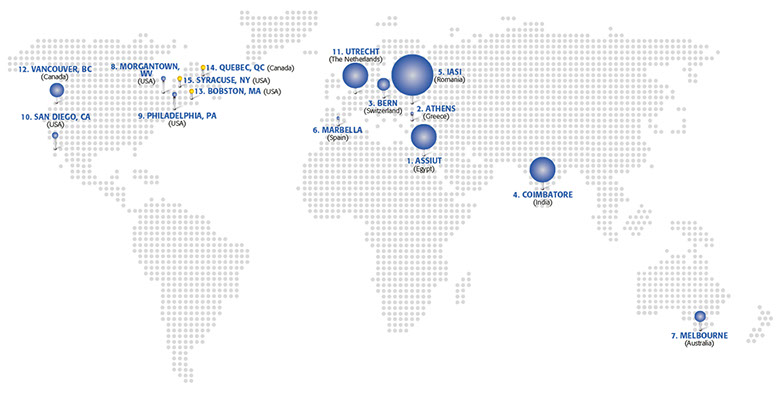
The participating sites were selected across the world through an open call to AOSpine members. A total of fifteen clinics representing four regions were finally included in the “We hope this study will give us clarity and understanding to why there is such a variation.”study: from Greece, the Netherlands, Romania, Spain, Switzerland, Egypt, Australia, India, Canada, and USA. “We included centers with different philosophies and everyone treats the patients as they think is best,” co-PI Cumhur Öner explains. “We are following these patients using the same terminology and same outcome instruments to create parallel cohorts of similar injuries treated in different ways. We hope this will give us clarity and understanding to why there is such a variation.”
In addition to Öner from the Netherlands, major contributors include Shanmuganathan Rajasekaran from India, and Mohammad El-Sharkawi from Egypt. El-Sharkawi's trauma center in Assiut receives 600 patients with thoracolumbar fractures each year, seven operating theatres running 24 hours a day through the week. Half of the injuries are caused “No patient should have to make a decision based on anything but solid knowledge.”by motor vehicle accidents. A high number of patients also come in after falling from heights on construction sites, due to poor safety measures. “Interestingly, in Switzerland we also get many high energy accidents, because we are so close to the mountains”, Lorin Benneker adds. On the other hand, North America and Europe have a growing number of osteoporotic fractures, which is an exclusion criterion in the study and adds to the challenge in recruiting patients in these regions.
By far the biggest contingent of patients—including the milestone one hundredth patient—has been recruited by Cezar Popescu from the “Prof. Dr. N. Oblu Emergency Hospital” in Iasi, Romania. Popescu's department annually admits up to 80 patients with such fractures, and he addressed the difficulties involved in recruitment early. “We knew our teams must really be ready anytime to properly examine the potential candidates, to explain the terms to the patients and their families, and to get written acceptance.”
Popescu is confident that the study will provide a better understanding of these lesions and give patients the correct treatment option. “No patient should have to make a decision based on anything but solid knowledge these days.”
AOSpine programs open research to new centers
Popescu's career inclined towards research through a fellowship in spine surgery in Budapest, Hungary, with the reputable AOSpine Knowledge Forum Member Péter Pál Varga as mentor. El-Sharkawi got into AOSpine research when the Assiut University Hospitals participated in a Research mentorship program. AO Clinical Investigation and Documentation (AOCID) organized training sessions and the team learned hands on research in the mentored PAM study.
“We had some challenges to match our data collection to the PAM study, but we managed. When recruitment in the Thoracolumbar Burst Fractures AOSpine A3/A4 study was slow “If I decide the patient may be treated conservatively, for sure, before he reaches home, someone else will suggest surgery.”and some centers were not coping, we were excited to join”, El-Sharkawi recalls confirming the clinical need. “This is a grey zone. If I decide a fracture is stable and the patient may be treated conservatively, for sure, before he reaches home, someone else will suggest surgery based on their experience”, El-Sharkawi explains and says patients are more likely to accept surgery. “Surgery is not as risky as before, patients become suspicious with other treatment options. Only with solid data to rely on, we can make a change and avoid unnecessary surgery.”
El-Sharkawi hopes for more opportunities to work with international organizations in studies such as the Thoracolumbar Burst Fractures AOSpine A3/A4, and opportunities to mentor younger surgeons in how to perform clinical studies.
- Mohammad El-Sharkawi, Assiut University Hospitals, Assiut, Egypt
- Spiros Pneumaticos, University of Athens, “KAT” Trauma Hospital, Athens, Greece
- Lorin M. Benneker, Inselspital, Bern, Switzerland
- S. Rajasekaran, Ganga Hospital, Coimbatore, India
- Eugen Cezar Popescu, Prof. Dr. N. Oblu Emergency Hospital, Iasi, Romania
- Ana María Cerván, Hospital Universitario Costa del Sol, Marbella, Spain
- Jim Wee Tee, Alfred Health operating through the Alfred Hospital, Melbourne, Australia
- John C. France, West Virginia University Department of Orthopaedics, Morgantown, WV, USA
- Alexander R. Vaccaro, Rothman Institute, Philadelphia, PA, USA
- Richard Allen, University of California, San Diego Medical Center, San Diego, CA, USA
- Cumhur Öner, UMC Utrecht, Utrecht, the Netherlands
- Marcel Dvorak, Vancouver General Hospital, Vancouver, BC, Canada
- Stuart Hershman, Massachusetts General Hospital, Boston, MA, USA
- Jérôme Paquet, Hospital l’Enfant Jesus, Centre Univeritaire de Quebec, Quebec, QC, Canada
- William Lavelle, SUNY Upstate Medical University, Syracuse, NY, USA
The fifteen participating sites representing four AOSpine Regions are on target to enroll 208 patients by end of 2019. Pin size represents volume of patients recruited at study site. Yellow pins are study sites opening soon
The AOSpine Knowledge Forum Trauma sponsored study is performed with the AO Clinical Investigation and Documentation support. More information on the “Thoracolumbar burst fractures (AOSpine A3, A4) in neurologically intact patients: An observational, multicenter cohort study comparing surgical versus non-surgical treatment” ‑study can be found on: clinicaltrials.gov ![]()
For more information on KF Trauma and the ongoing studies, go to www.aospine.org/kf-trauma ![]()
Newsletter 17 | July 2018
Newsletter 17
July 2018
feature storIES